

Why Does Red Light Therapy Work?
And what it tells us about our environment.

Red light therapy appears to have an unparalleled capacity to improve health metrics. From sleep quality to skin health to wound healing to bioenergetic regulation, red light therapy seems to be an important piece of the health puzzle. And with few to no notable side effects so far discovered (just a dose-response curve of diminishing returns), we may be tempted to ask why we wouldn’t want to use this modality regularly. But I see that as the wrong question. I want to know why it works and what that is telling us.
But first of all, how does it work in the first place?
Red light therapy, also know as photobiomodulation (PBM) or low level laser therapy (LLLT) works by irradiation of the body using specific wavelengths of light. Most therapies use 660/670nm light (deep red) and/or 780nm light (near-infrared) to achieve the wide array of benefits. These wavelengths are not the only ones that can be used to improve cellular function and repair, they appear to just be the ones most used in the literature.1 Reviews by PBM experts have noted that there really is no functional difference between LLLT and PBM.

Red light therapy goes back decades, and arguably centuries. There is good reason to classify heliotherapy as PBM as these wavelengths in question are abundant in sunlight (even on cloudier days). It has been known that sunlight exposure could treat and even cure diseases such as tuberculosis, lupus vulgaris, psoriasis and of course, rickets.
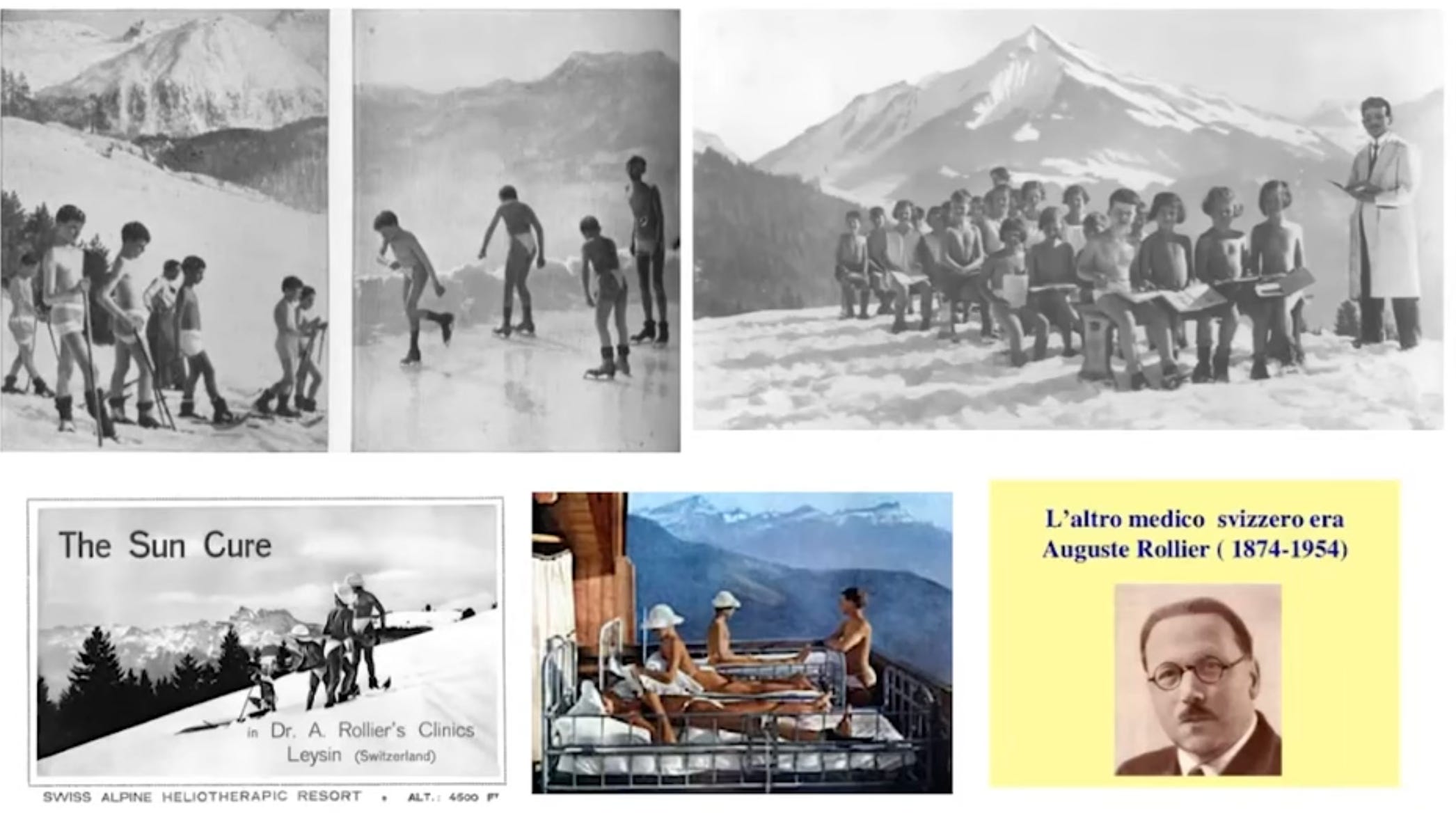
Although the method of action (obviously now we realise that methods of action is more correct) was unknown at the time, there wasn’t really any need to know; the fact that sunlight exposure worked was enough. Some nuance was added to this notion in European nations where there are sizeable portions of the year where the high-energy photons (UVB photons) are unable to traverse the ozone-rich atmosphere. Here, physicians set up clinics at high altitudes to increase the density of UV light that their patients could receive.
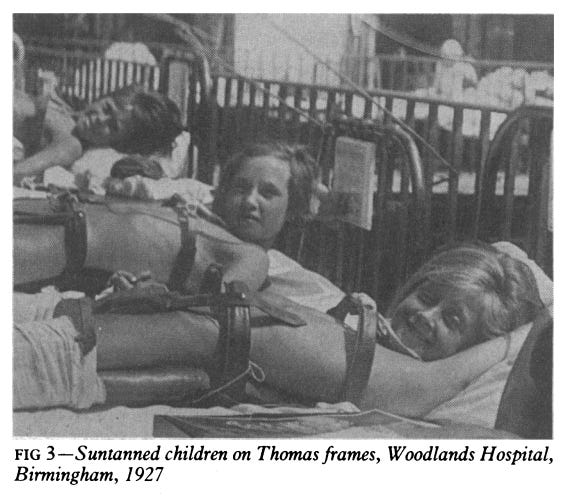
Clinics like these focussed on fresh air, cool temperatures and full-body exposure to sunlight in order to treat bone diseases, skin diseases and miasma (a broad constellation of symptoms probably akin to chronic fatigue and anemia) with great success.
Over the years following the success of these clinics, medicine moved in a different direction, largely phasing out heliotherapy. As we know now, it is essentially never used and most doctors would suggest that practices like this will give you cancer, not improve your health. But there remained an intriguing yet niche group of researchers who continued studying the effects of various lights on human health. Incandescent light baths and ruby lasers were used for a number of different maladies and even to help people regrow hair.
In 1963, Paul McGuff successfully treated malignant tumours with lasers. Although these were melanomas from human origin in a hamster model, no doubt this work should have become more well-known and widespread. It did not garner much attention at all, instead only Endre Mester attempted to repeat this anti-tumor effect of ruby lasers. Mester’s custom laser, however, did not provide the same radiant energy output and were thus probably not a true replication of McGuff’s original experiments. Mester’s experiments failed to show the same results, however, he did note that these lower powered lasers were able to cause an increase in hair growth in the experimental mice.

So it was well known that light had tangible biological effects. But little was known about how to integrate this information in a world focussed on pharmaceuticals and reductionism.
